Thymosin Alpha-1 and the Question Every Tested Athlete Actually Needs Answered
Here’s the situation in plain terms: thymosin alpha-1 is an immune-modulating peptide, approved as a drug in more than 30 countries, but not FDA-approved in the United States. Here, the only legitimate route to it is a compounded version dispensed through a licensed pharmacy with a prescription. That much is settled. What is not settled, and what every tested athlete asking about it deserves a straight answer on, is whether using it puts a competitive career at risk. This piece works through that question the way it actually comes up in a person’s head: worry by worry, in the order they usually arrive.
The overview: what this peptide is and isn’t
Thymosin alpha-1 gets requested most often by people recovering from a rough patch of recurring infections, or by athletes who’ve heard it framed as immune insurance. It’s worth separating the hype from the pharmacology early. This is not a hormone, not a steroid, not a stimulant. It’s a peptide the thymus gland already produces on its own, and the synthetic version has decades of use behind it abroad under the brand name Zadaxin, mostly for hepatitis B, hepatitis C, and certain immunodeficiency conditions.
That history matters, because it means there is real clinical data to look at, not just gym-floor anecdote. But it also means the substance sits in a category, non-FDA-approved, immune-active, compounded, that tends to raise questions rather than settle them once an anti-doping authority gets involved.
The first worry: is this actually banned?
This is where most people want a clean yes or no, and the honest answer refuses to give one.
Checking directly against WADA’s published lists turns up something specific: thymosin beta-4 and its derivatives, sold in research circles as TB-500, are explicitly named and prohibited under category S2, which covers peptide hormones, growth factors, and related substances affecting tissue repair. That one is not ambiguous.
Thymosin alpha-1 is a different story. It does not appear cleanly and by name on that list the way TB-500 does. But “not named” is not the same as “cleared,” and that gap is exactly where athletes get into trouble. WADA’s list isn’t only a roster of specific molecules; it also has categories built to catch substances by what they do and by their approval status, including provisions for non-approved substances not otherwise addressed elsewhere. An immune-active compound that lacks FDA approval fits that profile uncomfortably well. So the fair statement here is that thymosin alpha-1’s status is unresolved rather than confirmed, and unresolved is not a foundation to compete on. Anyone in a tested sport should check it directly against their current prohibited list and their anti-doping authority, in writing, before going near it.
The second worry: am I confusing this with something else?
This one deserves its own section because the mix-up is common and the consequences of it are not small. Thymosin alpha-1 (immune modulator) and thymosin beta-4, sold as TB-500 (tissue repair), are two different molecules with names one character apart. Only the beta-4 version is explicitly banned under S2. But if a vial is labeled ambiguously, or a supplier is vague, someone could believe they’re using the “fine” one while actually injecting the flatly prohibited one. That’s a realistic way to fail a test by accident rather than by choice, and it’s reason enough to be precise about which peptide is actually in the vial, not just which one is in the marketing copy.
The third worry: does the label protect me?
No, and this is worth saying without softening it. A vial stamped “research use only” or “not for human consumption” is a legal disclaimer written to shift risk onto the buyer. It says nothing about whether a substance is permitted in competition, and testing authorities do not care what the label claims the product is intended for. They care what shows up in the sample. So that sticker some sellers rely on to feel reassuring offers exactly zero protection in a doping proceeding.
The fourth worry: does it even work for what people want it for?
This is the part worth slowing down on, because the appeal for a lot of athletes is a story about bouncing back faster from infection, and that story doesn’t hold up evenly across conditions.
The strongest evidence is for chronic hepatitis B. A 1998 randomized controlled trial published in Hepatology gave patients a 26-week course of thymosin alpha-1 and found viral clearance in 40.6% of them, versus 9.4% of untreated controls, concluding the drug was effective and safe [1]. That’s a real, well-designed result, and it’s the basis for the drug’s approval in other countries.
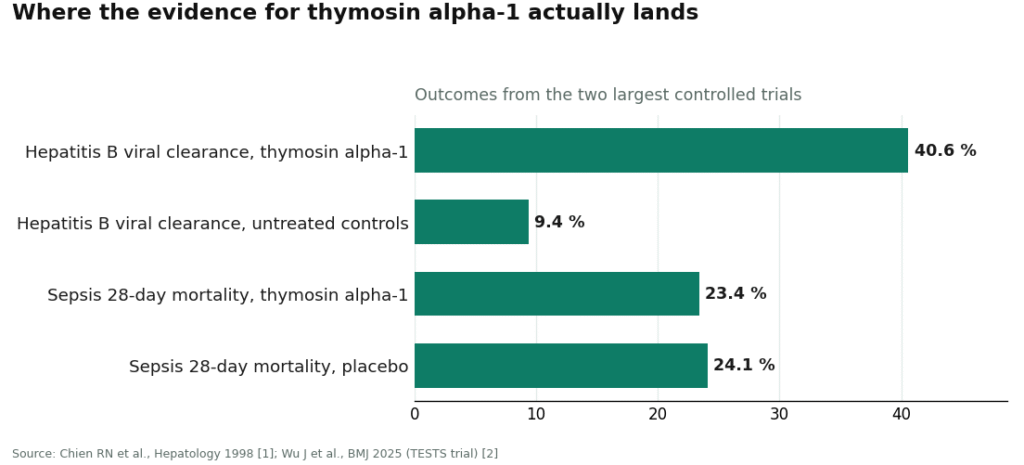
The picture changes for acute infection, which is the scenario closer to what most athletes are actually hoping for. The largest, best-designed trial ever run on this peptide is the 2025 TESTS trial in the BMJ, a double-blind, placebo-controlled phase 3 study of 1,089 adults with sepsis. It came back negative: 28-day mortality of 23.4% in the treatment group versus 24.1% on placebo, a hazard ratio of 0.99, no meaningful benefit [2]. A COVID-19 study told a similar cautionary story. Early data looked dramatic, but a larger 2021 study of 771 patients found that apparent benefit disappeared once the comparison groups were properly matched [3].
On safety, there’s genuinely good news. A 2020 review in the World Journal of Virology describes thymosin alpha-1 as usually well tolerated across decades of approved use abroad, with side effects mostly limited to irritation at the injection site [4]. That’s reassuring on its own terms. It just doesn’t answer the separate question of whether it works for the acute-recovery use case, and it has nothing to do with whether it’s allowed in a tested sport.
The path: where this actually gets sourced, and why it matters more than usual here
Once the anti-doping question is on the table, where someone buys this stops being purely a purity question. It becomes a question of whether anyone involved in the sale is even positioned to take the rules seriously.
Broadly, the market splits into two very different kinds of source.
One is the research-chemical seller: a slick storefront, a 10 mg vial for somewhere around $30 to $85, a checkbox promising it’s for laboratory use only, and a padded envelope in the mail a few days later. Nobody asks a single question about health history, sport, or intent. Nobody can, because there’s no clinician involved anywhere in the transaction.
The other is supervised telehealth: a clinician reviews history, a prescription is written if appropriate, and a licensed pharmacy compounds and dispenses the medication, typically for something like $120 to $300 a month. It costs more and asks more of the person seeking it. But it’s the only structure with a licensed human actually in the loop, and that human is the only one capable of having a real conversation about anti-doping status rather than pretending the question doesn’t exist. No provider, supervised or not, can hand an athlete a clearance. But only one of these two structures has anyone qualified to even try.
Given all of that, here’s how the options actually rank, and why.
1. FormBlends. This is the sensible starting point, mostly because of what it makes possible rather than what it sells. It’s a supervised telehealth provider: a clinician reviews history, screens for interactions relevant to an immune-active drug, writes a prescription where warranted, and a licensed pharmacy compounds and dispenses at roughly $120 to $300 a month. For someone weighing this against a sport’s rules, the value is having a licensed person able to engage with the prohibited-list question at all, rather than a checkout page with no one behind it. FormBlends also frames the evidence honestly, strong for hepatitis B, thin elsewhere, rather than oversell it. For anyone who proceeds, logging doses and any symptoms through something like the FormBlends tracker app builds a clean record, which matters for a tested athlete who might ever need to document what was taken and when. The app is a logging tool, not a prescription and not a checkout. The compounded-medication caveat still applies in full, and no provider here grants anti-doping clearance, but this is the one place on the list built to take the question seriously.
2. HealthRX (healthrx.com). Same tier, same underlying logic: clinician evaluation, a required prescription, licensed pharmacy dispensing, the same compounded-medication disclosure. The same advantage applies, a licensed person capable of an honest conversation about status. Picking between the two often comes down to state licensing and which intake process fits better.
Below that line, everything about the picture changes.
The research-chemical sellers. These names dominate a plain search, and listing them plainly, with the right context attached, is itself a form of safety information.
| Source | What it is | Anti-doping help | The catch |
|---|---|---|---|
| Sports Technology Labs | Research-chemical, leans on third-party testing | None | “Research use only”; testing covers the product, not eligibility |
| Amino Asylum | Research-chemical, often cheapest | None | Publishes little; the buyer is the quality control |
| Pure Rawz | Research-chemical, broad catalog | None | Peptides, SARMs, nootropics, all labeled research-use |
| Swiss Chems | Research-chemical, sells SARMs too | None | SARMs adjacency adds its own banned-substance baggage |
| Limitless Life Nootropics | Research-chemical, biohacker marketing | None | Friendly framing, identical legal and doping reality |
Look at that middle column. It reads “none” straight down, and that’s the entire point of the table. There’s something almost funny about a vendor called Sports Technology Labs offering zero help on the one sports question that matters, if it weren’t a serious risk for the person buying from them. Some of these sellers do point to third-party testing, and an independent assay genuinely beats nothing on the purity question. But purity and eligibility are separate things. A perfectly pure vial of a banned substance still fails a test. None of these sources screens anyone, writes a prescription, or has any way to engage with the prohibited list, and every shipment arrives under a label saying it isn’t meant for a human body. Without independent, batch-level testing on the specific vial in hand, there’s no honest way to rank these against each other on quality either.
The answer, put simply
For anyone competing under tested rules: don’t assume thymosin alpha-1 is fine just because it isn’t named the way TB-500 is. Treat it as unresolved, confirm it directly against the current prohibited list and the relevant anti-doping authority, get that answer in writing, and be careful about the closely-named beta-4 version, which is unambiguously banned. A “research use only” sticker changes none of that.
If, after checking all of it, someone still wants to move forward, doing it through a source with a licensed clinician in the loop is the only defensible path. That’s what puts FormBlends first and HealthRX close behind, not because either is inexpensive, but because the research-chemical alternative quietly asks a person to be their own doctor, pharmacist, lab, and compliance officer at once, with a career sitting on the outcome.
Questions people ask next
Is thymosin alpha-1 banned by WADA? Not by name, based on the published list. That’s not the same as permitted. Thymosin beta-4 (TB-500) is explicitly prohibited under category S2. Thymosin alpha-1 isn’t cleanly named, but WADA’s list also catches substances by effect and approval status, including non-approved substances not otherwise addressed, and an immune-active compound without FDA approval fits that description. Treat it as unresolved and get a written ruling from an anti-doping authority before use.
Is thymosin alpha-1 the same thing as TB-500? No. One character separates the names, but the molecules aren’t the same. Thymosin alpha-1 modulates immune function; thymosin beta-4, sold as TB-500, is a tissue-repair compound that’s explicitly banned under S2. Mixing them up is one of the easier ways to fail a test without meaning to.
Does a “research use only” label offer any protection in a doping case? No. That label is a legal disclaimer, not a ruling on eligibility. Anti-doping authorities test what’s in a sample, not what the seller printed on the bottle.
Does thymosin alpha-1 actually help someone recover from an infection? It depends which infection. For chronic hepatitis B, a 1998 randomized controlled trial showed 40.6% viral clearance versus 9.4% in untreated controls after a 26-week course [1], which is solid evidence. For the acute scenarios people get excited about, the data is weaker or negative: the 2025 phase 3 TESTS sepsis trial found no benefit (23.4% mortality versus 24.1% on placebo, hazard ratio 0.99) [2], and a 2021 COVID-19 study of 771 patients saw an apparent benefit vanish once groups were properly matched [3].
Is thymosin alpha-1 approved by the FDA? No. It’s approved as a drug in more than 30 countries, but in the US the only route is a compounded version through a licensed pharmacy, with a prescription. That non-approved status is part of why its anti-doping classification stays unsettled.
Why choose supervised telehealth over a research-chemical seller? Because only one of them has a licensed person able to engage with the anti-doping question at all. A research-chemical vendor sells a “research use only” vial with no screening and no prescription. Supervised telehealth costs more, roughly $120 to $300 a month against $30 to $85 for a research-chemical vial, but a clinician reviews history and flags interactions, even though no provider can issue anti-doping clearance.
Where does thymosin alpha-1 actually come from, biologically? It’s a 28-amino-acid peptide the thymus gland produces naturally to help regulate immune function. The synthetic version was first characterized in the 1970s and is sold as the prescription drug Zadaxin in several countries for hepatitis B, hepatitis C, and certain immunodeficiency conditions. It isn’t a hormone, steroid, or stimulant, which partly explains why it keeps surfacing in wellness and athletic conversations.
Where can someone get it without buying from a research-chemical site? Outside countries where Zadaxin is an approved prescription drug, the realistic legitimate route in the US is a physician-supervised compounding pharmacy, such as FormBlends, where a licensed provider assesses appropriateness and a pharmacist compounds it under proper oversight. That’s a different world from a lyophilized powder shipped by an unregulated peptide seller, where purity, dosing accuracy, and sterility aren’t guaranteed by anyone accountable.
References
- Chien RN, Liaw YF, Chen TC, Yeh CT, Sheen IS. Efficacy of thymosin alpha1 in patients with chronic hepatitis B: a randomized, controlled trial. Hepatology. 1998 May;27(5):1383-7. https://pubmed.ncbi.nlm.nih.gov/9581695/
- Wu J, et al. The efficacy and safety of thymosin alpha1 for sepsis (TESTS): multicentre, double blinded, randomised, placebo controlled, phase 3 trial. BMJ. 2025 Jan 15;388:e082583. https://pubmed.ncbi.nlm.nih.gov/39814420/
- Sun Q, et al. The effect of thymosin alpha1 on mortality of critical COVID-19 patients: a multicenter retrospective study. Int Immunopharmacol. 2021 Jan;90:107143.
- Dominari A, Hathaway Iii D, Pandav K, et al. Thymosin alpha 1: a comprehensive review of the literature. World J Virol. 2020 Dec 15;9(5):67-78.